

I recently wrote about my new Type 1 Diabetes diagnosis, the quest for affordable meds and supplies, and the subsequent financial savings found through transparent pricing outside of my insurance plan. I summarized that health care “coverage” is very expensive, whereas medical services may be found much more affordably.
My next step was to establish an ongoing primary care physician relationship. I contacted one of the large medical groups that my insurance plan covers and found that before meeting with the internal medicine physician, I would be required to have two visits with a physician assistant first. In regarding this option, I considered: (1) it is not unreasonable for me to seek direct access to a physician rather than being filtered through a physician extender, (2) especially in light of a new and significant medical diagnosis, (3) it is reasonable to anticipate having a personal relationship with my PCP, which would be hampered if I can’t meet him or her for another 6 months or more, (4) I am paying significant premiums for insurance “coverage” that I expect to purchase me access to physician services, and (5) being a physician myself, I want the expertise of a fully-trained, board-certified specialist that exceeds my level of training in general adult medicine. None of this is to denigrate our PA or NP colleagues who are integral to the team approach of medical service provision, but that is not the level of care that I choose to purchase as my initial consultation. (I’m sure that some would disagree with my opinion, but that topic is a debate for another time.)
Having previously visited a specialist in the above-mentioned medical group, I knew that new-patient and follow-up visits would likely approximate the specialist bills that I’d received: $285 and $127, respectively. After insurance “adjustments,” my out-of-pocket co-payments had been $166 and $87, respectively. Now, able to judge costs and service level of that PCP option, I compared these to a Direct Primary Care (DPC) practice that my daughter, Aubrey, had recently joined: Gentile Family Direct Primary Care (pronounced Jin-TIL-ee), in Pittsburgh, PA. I have keenly followed the DPC trend for several years, but this would be my first foray into the field as a patient.
Dr. Natalie Gentile’s initial fee is $100, followed by a $70/month membership fee. Some of the benefits of joining her DPC practice include: same or next day appointments of no less than 30-minutes duration; unlimited office visits with her; direct phone, text and email communication; and wholesale pricing for lab work, medications and many diagnostic tests. I ran the numbers, then emailed her for an appointment.
My first visit with Dr. Gentile lasted an entire hour as she not only focused on my medical issues, but on broader lifestyle, diet and family details. She subsequently researched and emailed me options for wholesale insulins and medical supplies. She saved me several hundred dollars over average retail pharmacy pricing on medications that were not covered by my insurance. Even had my insurance covered those meds, the “discount” would not kick in until I met my $3,000 deductible.
Given my busy work schedule during the week, I was not available to pick up my medications and supplies during office hours, and did not want them mailed to my home to sit on my front porch. Dr. Gentile stayed in frequent email contact with me, and offered to meet me on a Sunday afternoon so I could retrieve my meds! Needless to say, I have found my Primary Care Home.
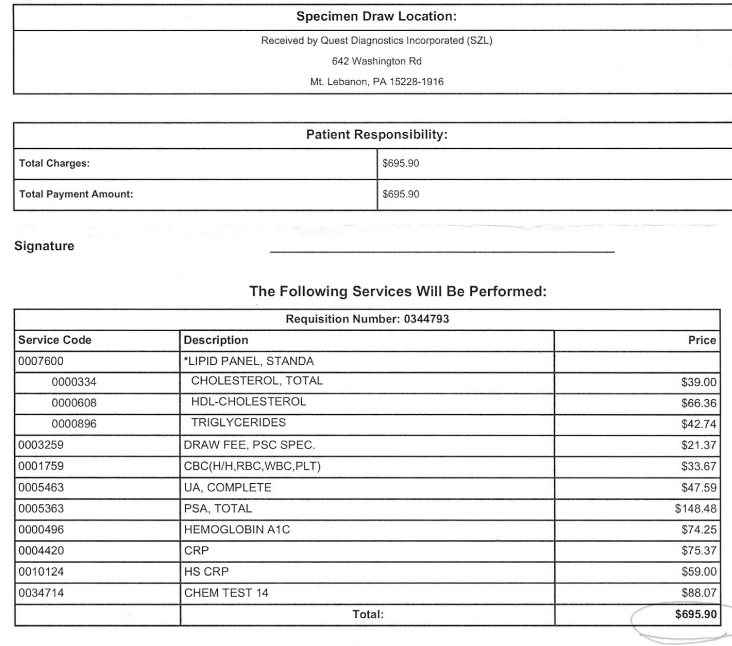
As I’ve promoted the idea of DPC, one of the concerns that I hear, and have had myself, is that the monthly membership fee might make the economics of the model unsustainable for patients. I calculated my own recent and projected medical expenses to get a comparison between insurance or retail pricing versus Dr. Gentile’s transparent wholesale pricing for visits and services. I project that in a year of quarterly “insured” PCP visits, I’d likely spend over $400 out-of-pocket, whereas with Dr. Gentile, I’ll spend over $900. However, comparing my recent lab work costs, I would have saved about $450 had she drawn the labs for me. Her wholesale prescription service will also save me at least $300 over a year compared to average retail prices. All told, I estimate a net savings of over $400 this year through my DPC membership. The potential for additional savings for other services is significant, particularly as I approach the age for screening colonoscopy – which she has coordinated for around $1,000 for her patients.
In summary, despite a monthly fee, DPC pays for itself (and then some) in many forms of savings and benefit. I believe DPC to be economically superior to the current third party payer model of medical practice. This is especially true for primary care and non-emergent outpatient medical services – which are arguably the majority of the demand in health care. I believe that DPC may be medically superior as this model allows physicians the time and flexibility to know their patients and accommodate their needs. DPC may also be superior from inter-personal, personal satisfaction, and humanistic aspects as the rushed, frustrating (for doctor and patient), insurance-restricted, 10-minute visit is replaced with greater availability, depth, flexibility, frequency and duration of interactions. Lastly, I consider the non-transparency of pricing in our profession to be a moral affront against the patient-consumer who has little idea of his financial obligation or exposure until after the fact. I can think of no other service or product line with similarly hidden and confusing costs. I have not found my own path to higher moral ground as a physician provider, yet, but I’m pushing us all towards greater awareness of costs and of systemic obstacles to transparency. For myself, as a patient, Direct Primary Care is a great stride forward.











{kind=link}