LAPD focused on peaceful protesters while ignoring looting, business owners say
In other words, those were their orders. Wonder why…

LAPD focused on peaceful protesters while ignoring looting, business owners say
In other words, those were their orders. Wonder why…
I wanted to write down and submit to the Libertarian Institute what I saw today at the protest in downtown Pittsburgh over the George Floyd killing. Some background on me: I am a Libertarian—a minarchist, not an anarchist. I was brought into the movement by the Ron Paul campaigns, and by reading Albert J. Nock, Rothbard, etc. I am a teacher by profession. I went to the protest because the killings of Floyd, Breonna Taylor, and Duncan Lemp are outrageous and wrong.
 The protest started off in downtown Pittsburgh, at Sixth and Liberty. When I got there, the march was just getting started, and the numbers were really substantial: in the thousands, for sure. The crowd was about what you would expect. A goodly number of African Americans of all ages, but skewing younger. Also present were a good number of white people, maybe half the crowd—also mostly millennials and younger. There were commies present, of course—scores, anyway, of crust punk, Antifa types. There was at least one red flag, and a guy handing out flyers on the necessity of socialist revolution. But needless to say, anarcho-communists were nowhere near the majority of marchers. There was an African American doing open-carry of an AR-15.
The protest started off in downtown Pittsburgh, at Sixth and Liberty. When I got there, the march was just getting started, and the numbers were really substantial: in the thousands, for sure. The crowd was about what you would expect. A goodly number of African Americans of all ages, but skewing younger. Also present were a good number of white people, maybe half the crowd—also mostly millennials and younger. There were commies present, of course—scores, anyway, of crust punk, Antifa types. There was at least one red flag, and a guy handing out flyers on the necessity of socialist revolution. But needless to say, anarcho-communists were nowhere near the majority of marchers. There was an African American doing open-carry of an AR-15.
The march wound its way through downtown, and although when I walked back through the route afterwards I saw evidence of tagging, I saw absolutely no property crime of any kind. I saw no violence, no scuffles, no confrontations, no theft, no looting, nothing of the sort. The march was entirely peaceful. We passed dozens of stores, hotels, and so forth. Nothing was touched.
I also saw no police, not one cop, until almost the end of the march. The march made its way to Washington Place, past the PPG Arena where the Pittsburgh Penguins play hockey. It halted around the intersection of Washington Place and Centre Avenue, near the beautiful Epiphany Roman Catholic Church.
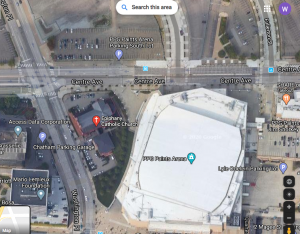 The march ended well East of where it had begun. To describe the area, Washington Place is a North South road which rises from a depression in front of the main entrance to the PPG arena North to meet Centre Avenue. Past the PPG arena on the west side of Washington Place is a business building that has the Mario Lemieux Foundation, among other things, and a parking deck with a railing that rises over the depression. On the East side of the street past PPG Arena is Epiphany Church. Washington Place rises to meet Centre Avenue, and the protest, after pausing in front of the main PPG Arena entrance on Washington Place, wound up the road and spread from PPG Arena onto Centre Avenue. Beyond Centre Avenue to the north is a vast open area of parking. The protest was pretty contained at this point. There is nothing much to the North of Centre Avenue at that intersection.
The march ended well East of where it had begun. To describe the area, Washington Place is a North South road which rises from a depression in front of the main entrance to the PPG arena North to meet Centre Avenue. Past the PPG arena on the west side of Washington Place is a business building that has the Mario Lemieux Foundation, among other things, and a parking deck with a railing that rises over the depression. On the East side of the street past PPG Arena is Epiphany Church. Washington Place rises to meet Centre Avenue, and the protest, after pausing in front of the main PPG Arena entrance on Washington Place, wound up the road and spread from PPG Arena onto Centre Avenue. Beyond Centre Avenue to the north is a vast open area of parking. The protest was pretty contained at this point. There is nothing much to the North of Centre Avenue at that intersection.
I walked up Washington Place to look at the carvings on the Church. I could see down into the depression. The crowd seemed to be moving North, so I did too. As I took a right from Washington Place onto Centre Avenue, I noticed—of all things—a parked police car. This was really odd. It was not blocking the street so demonstrators could march. The lights were not on. There was no cop with the car. Just the police car, parked there, by itself. I thought to myself at the time, “Man, I wouldn’t leave this police cruiser here, not with this march going on.” I figured it might get tagged. I kept walking East up Center Avenue.
There is an elevated place behind PPG arena on Centre Avenue where I went and stood behind a railing to watch. At this point, there was no violence. Police were visible on horseback, but they had withdrawn East up Centre Avenue as the protest emerged out of Washington Place and onto Centre Ave. People were milling around chanting. I noticed that one dude was eating a peanut butter and jelly sandwich out of a Ziploc bag, which was sort of charming. Then things got nuts.
As I am reconstructing this in my mind, knowing the fragility of eyewitness testimony, I am being as accurate as I can. I am being careful because what I saw next, I am convinced, was the police deliberately provoking the crowd. It was astonishing. Again, nothing destructive had happened yet. At this point, four police officers on horseback rode briskly through the crowd, moving downhill, East to West, on the sidewalk on the South side of Centre Avenue. The police on horseback were yelling instructions, but all four of them were yelling at once, and yelling different things. If they were ordering people to disperse, it was unclear. I could not understand a word of what they were saying—and they rode right past me, very close, as I watched on that slight rise behind the PPG arena behind a railing. No one was doing anything wrong, so it seemed needlessly confrontational.
This provoked a negative response further down to the West on Centre Avenue, and I heard, but could not see, clashes with the horseback police as they seemed to move first west then northwest. I cannot tell you what the protesters did, because I heard trouble, yelling and such, but my view was blocked.
Then, I saw the damndest thing I think I have ever seen. A police cruiser, lights on, sirens screaming, horn blasting, drove west down Centre Avenue toward the backs of protesters who were themselves facing westward further down Centre. A twenty-something black male ran in front of the police car, giving the black power salute, and the police cruiser jammed on the brakes and stopped. This caused twenty or so protestors to run toward the car and begin beating the sides of it. Another protester (stupidly, in my view) stood behind the police cruiser, preventing him from backing up. The police cruiser then slammed over the divider between lanes, and retreated at high speed. At that point, a hundred or so protestors who had run up when they heard the screeching brakes began chasing the police car. It stopped, then retreated again.
I asked the African American lady next to me what was happening—I figured I had to have missed something, some violence maybe, or some order to disperse that I had not heard. She responded, with an exasperated sigh, something to the effect of: “See how they do? It’s on now.”
And she was right. I figured this was going in a bad direction, and it was not like anyone was giving speeches or anything, so I decided to head back toward downtown. I went down Center Ave on the North side of the street watching the demonstrators. I stopped and got water out of my backpack, and looked to see where the horse cops went (I didn’t see them). After waiting a few minutes, I noticed the crowd surge toward that parked, solitary police car I had noticed when I walked past earlier. I saw that it had been tagged all over with paint. Then I realized a window had been broken and smoke was just beginning to come out. Somebody had just set the police car on fire.
 Crowds behave stupidly. As I was walking away an African American demonstrator with dreadlocks was yelling and pushing people away from the car: “Y’all know that’s gonna explode—get back, get back.” Thanks to his quick thinking and willingness to assert himself, the crowd wandered a safe distance away. By the time I got to the bridge on Centre after the intersection with Washington going West, small explosions started from the car. A police officer was standing at the intersection where the bridge starts—no riot gear, short sleeves—and no one was bothering him. I short time later, I noticed the riot cops were also on the scene, charging northward, uphill on Washington Place. I went back to my car and drove home.
Crowds behave stupidly. As I was walking away an African American demonstrator with dreadlocks was yelling and pushing people away from the car: “Y’all know that’s gonna explode—get back, get back.” Thanks to his quick thinking and willingness to assert himself, the crowd wandered a safe distance away. By the time I got to the bridge on Centre after the intersection with Washington going West, small explosions started from the car. A police officer was standing at the intersection where the bridge starts—no riot gear, short sleeves—and no one was bothering him. I short time later, I noticed the riot cops were also on the scene, charging northward, uphill on Washington Place. I went back to my car and drove home.
The explanation that the Pittsburgh PD has given on the evening news here is that a bad element hijacked a peaceful protest. That is partly true. The very large protest was peaceful as it wound through downtown. I will concede that from the beginning it was clear that Antifa/crustpunk types were there, ready to fight—bike helmets, goggles, designated first aid folk, etc. But they were nowhere near the majority, and until the cops first rode through—then damn near drove through—the crowd, even the Antifa types were behaving. No one was being violent or destructive. After those two police-driven incidents, as the young lady at the railing said to me, it was on.
I have radical politics, I guess, but I live a very conventional life. I suppose I am a “right-libertarian.” Before today, if you had told me you went to a demonstration, and the police had provoked a riot, I would have had a very hard time crediting that. “What would their motivation be? Why?” I am still trying to figure that out now. I really have no idea. However, I would swear up and down, in a court of law if I had to, that the cops provoked the rioting in Pittsburgh today. They turned a peaceful, if angry, atmosphere into to the fearful, raging, confrontational crowd that Antifa could then steer into property crimes and violence. And they did it right in front of my eyes. None of that excuses Antifa. I don’t like commie violence against property any better than anyone else who follows the Libertarian Institute, and apparently after I left for my vehicle on the other side of downtown, they started breaking windows and attacking people’s private property.
But, as crazy as it sounds, the cops started it. I was there. I saw it.
Doing his best impression of Bush and Cheney on September 11th, Trump flees in cowardly terror to his underground bunker due to protests and riots outside.
As though 1 the protesters had any intention of storming the White House and lynching the president or 2 that the cops and soldiers on premises would be unable to stop them if they tried.
Surprised that Mr. All Politics is Daytime Cable News would seek to portray himself as such a weak, fearful little girl at a time like this, but he is what he is.
More of Susan Rice speculating on CNN that Russia is fueling US protests: "I would not be surprised to learn that they have fomented some of these extremists on both sides using social media. I wouldn't be surprised to learn that they are funding it in some way, shape, or form." pic.twitter.com/qLGdZuxBuo
— Aaron Maté (@aaronjmate) May 31, 2020
Of course. America is already great. Now if only the terrible Russians didn’t control all of our minds, then we’d finally be happy!
This week, I am introducing the Ending Qualified Immunity Act to eliminate qualified immunity and restore Americans’ ability to obtain relief when police officers violate their constitutionally secured rights. pic.twitter.com/PiNYP8cX8i
— Justin Amash (@justinamash) June 1, 2020
April 26, 1992. There was a riot on the street, tell me, where were you?
I get the feeling the majority of you rioting right now were either too young or not even born yet when that song made its rounds. Didn’t quite have the ability for those events to make their mark on your worldview.
Something tells me this event ends the same as that event.
I’m curious to see the ways in which this year gets neatly packaged and scripted into an overlooked little chapter to be taught to schoolchildren in 2050. I wonder, what will be the foundation of the narrative? What lessons will the government run public school systems be conveying when they discuss 2020 and the relationship a government holds with its constituency?
With any luck I’ll still be around to witness that. Why do I get the sense that it will be something that supports acquiescence to authority?
This is a bad time to write this piece. Perhaps the worst times to write something are the most effective? I don’t know.
I’ve been speaking out against and writing about police violence for many, many years. It’s on record. I supported Colin because he spoke out against the violence of the state, period. I supported BLM because they spoke out against the violence of the state. I may not agree with their interpretations of root cause, but regardless, a voice against the state is appreciated either way.
That is why I’m writing today.
Root causes.
Solutions.
Change.
The State’s violent enforcement of policies have claimed many, many lives. It always has. It hasn’t been until recently, 2013 I believe, that online resources began popping up to make an effort to officially track and tally these instances of violence. Before that, there was no reliable source of data whatsoever.
If you listen to the news. Most of those victims are black. They aren’t. Not even close. From Duncan Lemp sleeping peacefully in his bed to Kelly Thomas who apologized to officers 15 times while they literally beat him to death, there are heart breaking tales from all ethnicities, including 6 year old autistic boy Jeremy Mardis whose father was unarmed in the front seat of the car and even babies during SWAT raids. Derek Hale in 2007 sitting on his friend’s front porch getting up to help his friend’s girlfriend with her two kids. Stephan Cook forcibly raped by police in 2012. Nick Christie, whose wife mistakenly called police to inform them her husband had traveled to FL and forgotten his medicine, was accosted, hooded and pepper sprayed……to death. James Ahern who was unarmed and shot in the back in 2010. His assailant was promoted to Chief. David Eckert in New Mexico who was forcibly raped for having the nerve to ask if he was free to go.
I can keep going, there’s a never ending supply of these kinds of stories. The abuse is color blind, I promise you.
In the interest of time I decided to look back at the last 3 ½ years solely to see how many unarmed civilians were killed during an interaction with police. Only unarmed. That’s not to say that everyone who was armed deserved to be killed. Not at all. Some did, certainly. If you physically threaten another’s life, any individual has every right to defend themselves. Whether or not they are an officer is irrelevant.
In the interest of consistency, civilians have that exact same right and if a group of humans bust down someone’s door at 2 AM that person has every right to defend themselves as well and has every right to pick up their gun to do so. They don’t know those are police officers busting down their door.
In the last three and a half years I was curious in comparing deaths of unarmed civilians across White, Black and Hispanic lines. This count is not complete. There were quite a few victims who were never identified, and their race not confirmed. I left all those out of the count. I also left out Asians in my tally though there were a handful. Three or Four I believe.
The final count since 2017 of unarmed civilians: 24 Black : 25 Hispanic : 61 White
Now I know, the natural argument is to draw attention to the disparity in relation to population. That’s fair. Black Americans make up 14% of the US population and yet are 22% of unarmed victims. White Americans make up 60% of the US population and are only 55% of unarmed victims. You can make an almost identical observation if tallying all deaths due to police interaction and you can make a similar observation with respect to arrests as well I would bet. I’ve studied crime data extensively but haven’t seen a dataset that simply outlined arrest records by demographic.
That said, are we really stating that disparity is the cause of our pain? Really?
Do you mean to tell me that over the next 3 ½ years if the police have killed 110 unarmed civilians and 15 of them are black, 18 are Hispanic and 66 are White then there will be no riots in the street and you will interpret the world in which you live as just?
We don’t have a race problem in American policing. We have a prohibition problem in American policing.
You want to riot? You want justice? You want change?
GOOD! But……
We need coordinated action and goals. If this keeps up much longer here’s what’s going to happen.
You’re going to get tired of protesting. You’re going to get hurt. You’re going to get incarcerated. You’re going to lose your momentum. Your anger is going to subside. George Flynn’s murderer is going to be indicted and that’s going to tell you that some kind of justice was eventually served and you’re going to get back to living your life.
Then, we can do this all over again in another 28 years when nothing of substance changed.
How do we not let that happen?
We need to reorient our law enforcement from the profitable and predatory practice of fighting the war on drugs at the behest of federal policies and back toward the actual practice of ensuring the safety of our citizens.
We need to know that the officers in our communities’ employ are dependable and respectable. The types of human beings that we could trust to ensure a safe community.
How do we do all this?
Well, as far as accountability goes, I would say let’s make police officers accountable. Seems easy right? I’m not talking about being charged with a crime after they do something horrendous. Though should they do something horrendous then that is obviously a crime, so please, charge them with one.
No, I’m talking about something much more basic. Personal liability.
If a plumber comes over and floods your entire house due to negligence or incompetence you have the just right to pursue compensation and damages. The plumber is required to carry insurance to cover their work.
If a surgeon paralyzes you due to negligence or malpractice you have the just right to sue for damages. Doctors carry enormous malpractice policies for just this reason.
Why not make police officers carry malpractice insurance? Personally. Fine, go to the academy, get all your training, accept your new role, oh, but before you are able to start on day one, you have to apply for and get approved for malpractice insurance. The monthly rate gets automatically drafted out of your paycheck.
Hell, police departments would even end up subsidizing the cost I’m sure.
But do you know what would happen? Insurance companies would police themselves. Just as they do with doctors and service providers. If an officer does something wretched and gets sued, then just like with your car insurance, their rate goes up. If it goes up high enough, eventually that officer prices themselves out of employment. Bad cops, gone.
This seems pretty obvious and I’m not the only one making the argument. I saw a fantastic article on this site two days ago promoting the same premise.
I’m willing to bet there are quite a few attorneys that are part of this movement no? Did you know the Supreme Court has historically overturned 236 of it’s rulings?
Create class action lawsuits against the United States. Sue against Qualified Immunity. A 1983 Supreme Court ruling that arbitrarily creates impunity for all government employees acting within the official capacity of their role. It’s the same doctrine that allows the people who poisoned me and so many other Vets to walk free.
Stand outside the Supreme Court the day of the ruling on that lawsuit ready to riot.
Create class action suits against the Civil Asset Forfeiture program that began in 1970. Wait outside the Supreme Court.
Create class action suits against the 1033 Program that funnels retired military equipment to local police departments.
Create class actions suits that challenge the legal capacity for police departments to continue with their practice of conducting over 50,000 SWAT raids per year. You read that correctly.
Create class action against Federal drug policies.
As far as the drug war goes, which was initiated around a foundation of systemic and institutional racism, make no mistake, is a little more complex and tricky.
There exists no one size fits all solution for this issue. Other than one aspect; Nullification.
States need to nullify federal mandates and create their own policies surrounding drugs and enforcement that are individually aligned with the communities they police. Beyond that, local cities need to nullify state mandates should they want to try something different as well. This is already happening with marijuana.
I don’t have all the answers, but I do know if 100 people try 100 different things then we’ll learn something as a society. And maybe even make progress.
This issue has always been vastly more socio-economic than it has been about race. I know for a fact that in the poor white neighborhoods where drug use is prevalent those communities are badgered by police to the same degree as poor black neighborhoods.
It’s time to change our relationship with the State and to the degree that law enforcement continues to exist, change our relationship with officers as well.
It is, after all, a decision that is ours to make. You’re the boss. Remind them of that.
Let’s create a new song this year. One that ends in change.
https://democracyjournal.org/arguments/the-war-on-drugs-has-made-policing-more-violent/
https://ij.org/report/policing-for-profit/
https://www.wsj.com/articles/the-underpolicing-of-black-america-1422049080
https://thecrimereport.org/2015/06/24/2015-06-reinventing-american-policing-a-seven-point-blueprin/
The War on Drugs is the immediate cause of, and pretext for, the system of oppression, and police violence and militarization.
Ending the War on Drugs is also a project that can unite rather than divide, something that people from different races and different ideologies can agree on and get behind.